Gallery











Onobotulinumtoxin A injection is an option for patients who have failed conservative therapies. The toxin is reconstituted in a small volume of sterile saline. We use 1 cc of normal saline to reconstitute 100 units. Onobotulinumtoxin A is injected into the fissure and internal sphincter. This procedure can be performed in the office or in the operating room with sedation for patients experiencing severe anal pain. The concentration, dosage of injection, and specific location of injections are surgeon dependent. There is a paucity of high quality studies that describe technique and support effectiveness. The pathophysiology is that Onobotulinumtoxin A causes temporary paralysis of the internal anal sphincter, reduces in anal sphincter tone, and promotes healing by increasing blood flow to fissure.Complications of this procedure are low, but the following has been reported: fecal urgency and incontinence, hematoma, proctitis, and injection site infection.
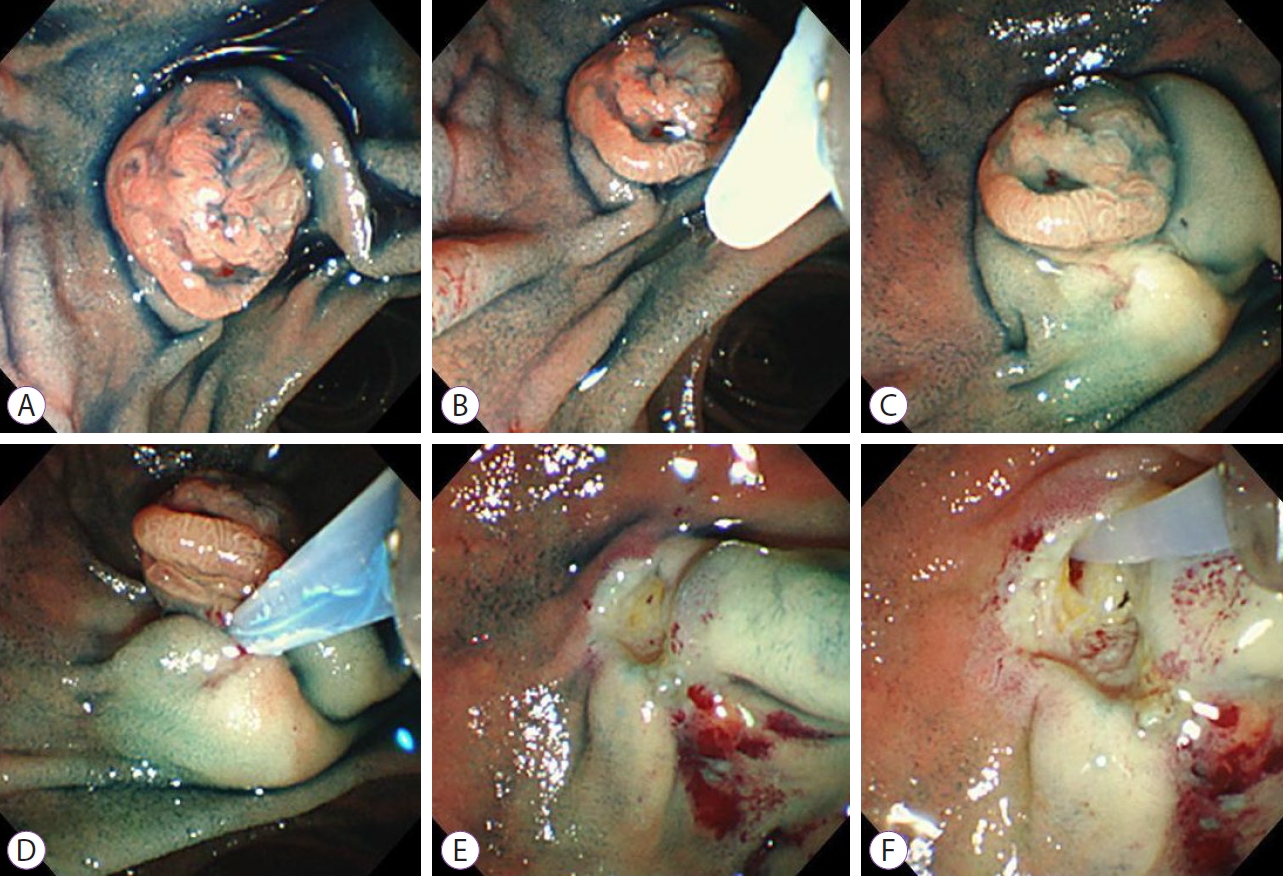
The patient was a young adult male with a history of chronic anal fissure with increased symptoms of pain and bleeding despite a prolonged course of conservative medical management. Patient received botulism toxin injection to reduce anal sphincter tone and promote healing of fissure. The Onobotulinumtoxin A was reconstituted by injecting 1 cc of injectable saline into the vial of 100 units. The 100 units was injected on either side of the fissure and in the intersphincteric groove on both the right and left sides for sphincter relaxation.
The indications for injection of the anal bulking agents in these studies were various. Most patients had passive FI, but some had urge incontinence, indicating EAS disruption. The results of these initial studies showed that continence was improved in the short term. However, the medium- and long-term results were poor, probably because of the resorption or migration of the injected material. Reinjection was necessary in order to maintain continence.
The bulking agent may be injected freehand, with an anal retractor such as Eisenhammer used to identify the IAS and intersphincteric groove. A finger placed within the anal canal may be useful to guide the needle to its correct position. However endoanal ultrasound has been recommended to guide the needle to an optimum position [], especially if the agent is to be injected into the intersphincteric space or adjacent to a defect in the IAS.
The majority of patients did not report any complications. The complications described were mainly pain, anal bruising and leakage of injected material [, ]. Less common complications were anal ulceration and infection (local cellulitis and abscess formation). There were two reported cases of local giant cell foreign body reaction after injection of silicone (PTQ) []. Durasphere has been associated with skin rashes and arthritis. Skin patch testing is therefore recommended before using this agent [].